
Thursday, 7 August 2014
Saturday, 18 May 2013
10 Reasons to Choose General and Business Transcription Work Instead of Medical Transcription
1. Work from home
2. Great income potential 3. Plenty of work available4. You don't need special training or certificate 5. You don't need to know medical terminology 6. You can start working almost immediately 7. Flexible hours and workload 8. Easy and inexpensive to start9. Get clients nationwide (and even worldwide) 10. Slower turnaround time than medical transcription |
 |
The General and Business Transcription
Biz-In-A-Box Start-Up Kit
The general and business transcription start-up kit makes it easy for you to get started. I'll take you step-by-step and show you how to get started. You'll get all the insider information you'll need to get transcription work from home and become a successful transcriptionist. By learning from my experience, you will become successful a lot faster than I did.
The four parts include:
|
Sunday, 24 March 2013
CPC Practice Exam Sample Questions
Example 1: Medical Terminology
The term "Salping-Oophorectomy" refers to
a. The removal of the fallopian tubes and ovaries
b. The surgical sampling or removal of a fertilized egg
c. Cutting into the fallopian tubes and ovaries for surgical purposes
d. Cutting into a fertilized egg for surgical purposes
Rational
Answer: A
The term "salp" means tube, the term "ooph" refers to the ovary, and the suffix "ectomy" means to surgically remove. Some CPT books (like the professional edition put out by the AMA) contains pages with common medical terms like these in the beginning of the book (prior to the coding guidelines)
Example 2: Musculoskeletal
OPERATIVE NOTE
PREOPERATIVE DIAGNOSIS: myelopathy secondary to very large disc herniations at C4-C5 and C5-C6.
POSTOPERATIVE DIAGNOSIS: myelopathy secondary to very large disc herniations at C4-C5 and C5-C6.
PROCEDURE PERFORMED:
1. Anterior discectomy, C5-C6
2. Arthrodesis, C5-C6
3. Partial corpectomy, C5
4. Machine bone allograft, C5-C6
5. Placement of anterior plate with a Zephyr C6
ANESTHESIA: General
ESTIMATED BLOOD LOSS: 60 mL
COMPLICATIONS: None
INDICATIONS: This is a patient who presents with progressive weakness in the left upper extremity as well as imbalance. He has a very large disc herniation that came behind the body at C5 as well and as well as a large disc herniation at C5-C6. Risks and benefits of the surgery including bleeding, infection, neurologic deficit, nonunion, progressive spondylosis, and lack of improvement were all discussed. He understood and wished to proceed.
DESCRIPTION OF PROCEDURE:
The patient was brought to the operating room and placed in the supine position. Preoperative antibiotics were given. The patient was placed in the supine position with all pressure points noted and well padded. The patient was prepped and draped in standard fashion. An incision was made approximately above the level of the cricoid. Blunt dissection was used to expose the anterior portion of the spine with carotid moved laterally and trachea and esophagus moved medially. I then placed needle into the disc spaces and was found to be at C5-C6. Distracting pins were placed in the body of C6. The disc was then completely removed at C5-C6. There was very significant compression of the cord. This was carefully removed to avoid any type of pressure on the cord. This was very severe and multiple free fragments noted. This was taken down to the level of ligamentum. Both foramen were then also opened. Part of the body of C5 was taken down to assure that all fragments were removed and that there was no additional constriction. The nerve root was then widely decompressed. Machine bone allograft was placed into C5-C6 and then a Zephyr plate was placed in the body C6 with a metal pin placed into the body at C5. Excellent purchase was obtained. Fluoroscopy showed good placement and meticulous hemostasis was obtained. Fascia was closed with 3-0 Vicryl, subcuticular 3-0 Dermabond for skin. The patient tolerated the procedure well and went to recovery in good condition.
a. 22554, 63081, 63082, 20931, 22845
b. 22551, 63081, 20931, 22840
c. 22551, 63081, 63082, 20931, 22845
d. 22554, 63081, 20931, 22840
Rational:
Answer: A
Per. Paul Cadorette and the American Medical Association article titles, "Coding Guidance for Anterior Cervical Arthrodesis", "When a spinal fusion (arthrodesis) is performed, the first thing a coder needs to recognize is the approach or technique that was utilized. With an anterior (front body approach)to cervical fusion the incision will be made in the patient's neck, so the key terms to look for are platysma, esophagus, carotid, and sternocleidomastoid. These structures will be divided and/or protected during dissection down the vertebral body. After dissection, the procedure can proceed on one of three ways:
1) When the interspace is prepared (minimal discectomy, perforation of endplates) then 22554 would be reported.
2) When a discectomy is performed to decompress the spinal cord and/or nerve root(s) report 22554 for the arthrodesis along with 63075 for the discectomy procedure.
3) When a partial corpectomy (vertebral body resection) is performed at C5 and C6 report CPT code 22554 for the arthrodesis with 63081 and 63082. Two codes are reported because the corpectomy procedure is performed on two vertebral segments (C5 and C6). CPT codes 63081-63091 include a discectomy above and/or below the vertebral segment, so code 63075 (discectomy) would not be reported if performed at the C5-C6 interspace.
Once the decompression procedure has been completed, a PEEK cage can be placed within the interspace or a structural bone graft can be fashioned to fit the vertebral defect created by the previous corpectomy. Insertion of the PEEK cage would be reported with a biomechanical device code 22851. This code is only reported one time per level even if two cages are placed at C5-C6. When a structural bone graft is used, determine whether it is an allograft (20931)) or an autograft (20938). The bone graft codes are only reported one time per procedure and not once for each level. Finally, the physician will place an anterior plate with screws (22845) across the C5-C6 interspace to stabilize the area fusion".
Some guidance on coding such procedures can also be located in the Spine (vertebral column) coding guidelines (above code 22010).
Example 3: ICD-9-CM
Jim was at a bonfire when he tripped and fell into the flames. Jim sustained multiple burns. He came to the emergency room via an ambulance and was treated for second and third degree burns of his face, second degree burn on his shoulders and forearms, and third degree burns on the fronts of his thighs.
a. 941.20, 841.30, 943.25, 943.21, 945.36, 948.42, E897
b. 941.30, 943.29, 945.36, 948.42, E897
c. 941.09, 943.09, 945.09, 948.64, E897
d. 941.30, 943.29, 945.36, 948.64, E897
Rational
Answer: B
Burn codes always have no less than three codes: A burn code, a total body surface area code (948.XX), and an E code. You can have more than three codes but never less. Burn codes have the following rules (which can be found at the beginning of the ICD-9 book under general guidelines), always code one location to the highest degree (Ex. 1st and 2nd degree burns on the arm, only code 2nd degree). When sequencing burn codes always list the highest degree first (Ex. 1st degree burns to the face and 3rd degree burns to the arm. List the arm burn first and then the face burn). Answer B is the answer because its codes describe the highest degree burn to each anatomical location, it sequences the burn codes in order of highest to lowest degree burns, the 948 (TBSA code) has the correct calculation, and the E code correctly describes the bonfire incident.
Example 4: Anesthesia
When does anesthesia time begin?
a. After the induction of anesthesia is complete
b. During the pre-operative exam prior to entering the OR
c. When the anesthesiologist begins preparing the patient for the induction of anesthesia
d. Once the supervising physician signs over the patient's care to the anesthesiologist
Rational
Answer: C
The answer to this question can be located in the anesthesia coding guidelines under the title "Time Reporting"
It's time to STOP doing what's not working, and get the CPC Practice Exam - fully updated in 2013!
Contents of the practice exam:
- 150 Question CPC Practice Test
- Answer Key, With Full Rationale
- Scan Tron Bubble Sheets
- The Exam Study Guide, including:
Common Anatomy Terminology Handouts
Common Medical Terminology Prefix, Root Word, and Suffix Handouts - The Official AAPC Proctor-to-Examinee Instructions (read out loud on the day of the exam)
AAPC's CPC exam is 150 questions long. Questions range from true and false, to 1-2 sentences, to full page operative notes.
Questions on the CPC exam do not cover just specific medical codes. Questions can be very diverse, testing the examinees knowledge on:
- Coding Guidelines
- Understanding of Conventions
- Correct Modifier Use
- Bundling and Global Packages
- Medical Terminology and Gross Anatomy
We have taken into account the wide spectrum of diversity the CPC exam offers and have constructed the questions on our CPC Practice Exam to reflect those on the actual exam as closely as possible.

**We'd like to thank MTSamples.com for providing some of the dictation for our operative report questions as well as the ASC Review for their coding guidance article by the American Medical Association.**
Starting A Home Based Medical Billing Business
What You Will Learn:

- The truth behind whether this business can be started without any prior experience in this field.
- How much money you will really have to invest into starting this type of home based business.
- How to avoid getting scammed and overwhelmed trying to get started.
- How to choose the best medical billing training program, school or correspondence course (on and offline) and exactly where to find them.
- What the best medical billing software packages are.
- What a medical billing opportunity is, where to find them and who to contact.
- Who the best medical billing clearinghouses are and why you need them.
- How long it will take you to get up and running.
- What the average medical billing salary for a home based medical biller is and what you can do ensure that the amount continuously rises.
- The how's and why's about the medical billing process and how to do it properly from home as a business venture.
- You'll have in your possession usable and printable examples of medical billing contracts, marketing fliers and other forms that you need to be familiar with.
- The correct way to choose a name for your business.
- How to set up your business entity legally in the eyes of the law (Corp., Inc., LLC., etc).
- What three services at a minimum you should be offering to prospective physicians.
- How to set-up and develop the pricing for your services so that you're profitable and competitive within the marketplace.
- What equipment you will need to do the job like a pro from your home.
- Where the experts go to network with other medical billers (new and old).
- Where the expert medical billers go when they have questions.
- What HIPAA is and why it impacts you as a medical billing business.
- What you must do to get doctors for your business and where to find their contact info.
- How and where to go to market your business and services.
- You'll know exactly what you should be saying to prospective physicians and their staff to secure their business (printable word-for-word scripts included).
- What kinds of paperwork you will need and where to go to download or purchase them.
- Most of all you will be able to decided based on facts if starting a home based medical billing service is the right business for you to undertake or if you should choose another!
Click Here to download this bible!
Pharmacy Technician Training & Orientation Course

RXinsider’s Pharmacy Technician Training & Orientation is a no-nonsense training program for anyone interested in a career within the pharmacy profession. The program focuses on basic skills and understanding while minimizing training burdens on the existing pharmacy staff. RXinsider’s Pharmacy Technician Training & Orientation is the perfect starting point for cross-training front store pharmacy personnel, training new pharmacy staff or self-directed training for individuals interested in becoming a pharmacy technician.
Can you decipher the following prescriptions?
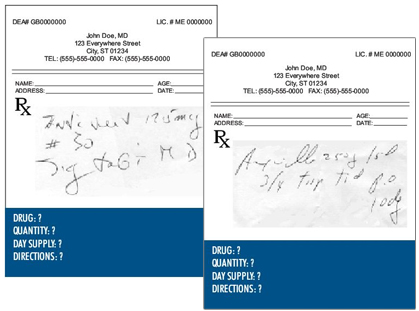
Can you calculate how long the prescription should last?
Can you read the directions?
…you will after completing RXinsider’s Pharmacy Technician Training & Orientation program.
- Four comprehensive and relevant modules
- Unlimited online access 24/7
- Assessment quiz & certificate of completion
- Web-based
- Affordable investment
By completing the training program, trainee should:
- have an idea of what a typical Pharmacy Technician's duties will entail.
- gain general and basic knowledge of a typical retail pharmacy and its operations.
- feel less overwhelmed and stressed during the first few weeks of employment.
- prove to future employers their commitment to becoming part of the pharmacy team.
- gain an edge on any other applicants for a particular pharmacy position.
- save time and frustration during the in-store training process.
- determine whether a career in pharmacy may be the right fit.
- NOTE: This program is NOT intended as a study guide for the PTCB Exam.
- General Pharmacy Information
- Sig Codes/Abbreviations
- Brand-Generic Name Recognition
- Prescriber Handwriting Recognition + Day’s Supply Calculations
- Self-Assessment Quiz
Subscribe to:
Posts (Atom)